Parotid gland
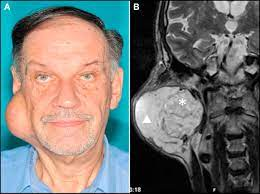
Before examination you should know the position of parotid gland- it lies below, behind & slightly in front of lobule of ear. A swelling of parotid gland thus obliterates the normal hollow just below the lobule of ear. Like any other swelling, the extent, size, shape, consistency, history of presenting illness etc should be noted.
History of presenting illness
In any illness or disease careful history must be taken.
In case of swelling, the following questions should be asked...
- How did the swelling start?
- Where exactly swelling first noticed?
- How long is the swelling present?
- Has the swelling enlarged uniformly throughout the period?
- Has it suddenly enlarged very recently?
In Acute parotitis- Patient will be dehydrated with poor oral hygiene, complains of sudden increase in size of both the parotid glands, with pain.
Parotid abscess- There is brawny edematous swelling of parotid region with pain.
Mikulicz's syndrome- There is generalized enlargement of all major salivary glands including lacrimal glands [If it associated with dry eyes & generalized arthritis then it is called Sjogren's syndrome].
Pleomorphic adenoma- slow growing tumor having duration for years or months of parotid gland.
In case of pain-
- Acute parotitis is painful.
- Parotid abscess- throbbing pain is characteristic feature, excruciating pain, slight swelling, & redness in region of parotid gland.
- In case of obstruction of parotid duct with stone or stricture patient will complain of colicky pain during meals when the swelling of parotid gland will also be increased.
Watery discharge from a sinus in the region of parotid gland or its duct particularly during meals is significant of parotid fistula.
Inspection & palpation
1) Swelling- whether swelling is fixed to masseter muscle or not is examined by asking the patient to clinch his teeth & the mobility of swelling is tested over the contracted masseter muscle.
2) Skin over the parotid gland-
- In parotid abscess the skin becomes brawny oedematous with pitting on pressure.
- It must be remembered that fluctuation is very late feature of parotid abscess as there is strong parotid fascia overlying the parotid gland. Skin will also be warm & extremely tender.
- One should also look for any scar or fistula in this region.
- When parotid malignancy is suspected careful examination must be made to exclude if there is infiltration of skin by tumor.
Location: The parotid (stensen's) duct starts just deep to anterior border of gland & runs superficial to masseter muscle, then it curves inwards to open on buccal surface of cheek opposite the crown of upper second molar tooth.
In case of suppurative parotitis, gentle pressure over the gland will cause purulent saliva to come out of the orifice of duct.
In case of malignant growth blood may be found.
While duct rounds over masseter muscle one can feel the duct by rolling the finger over the taut masseter muscle.
The terminal part of the duct is best palpated bidigitally between the index finger inside the mouth and the thumb over the cheek.
4) Lymph node examination- Preauricular, the parotid, submandibular groups of lymph nodes are mostly involved.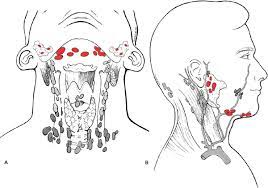
Movement of jaw restricted if growth is malignant & has involved the periarticular tissue of temporomandibular joint.
Differential diagnosis
Congenital sialectasis:
Dilatation of ductules & alveoli, occurring in one gland usually.
Symptoms occurred in infancy and characterized by attacks of painful swelling of parotid gland, often accompanied by fever.
Allergies to certain food also seen.
Diagnosed by sialography.
Calculus:
Rarely formed in parotid gland because secretion is watery.
Acute suppurative parotitis:
Infection reaches the gland from mouth and rarely it is blood-borne.
There is brawny edematous swelling over the parotid region with all signs of inflammation.
Fluctuation is a late feature due to presence of strong fascia over the gland.
The auriculotemporal (Frey's) syndrome:
This condition follows injury to auriculotemporal nerve while incising for suppurative parotitis.
At the time of meals, parotid region and the cheek region will become red, hot & painful, soon beads of perspiration appear on this area.
Cutaneous hyperesthesia is also present over this area & becomes evident to the patient while shaving.
Acute parotitis:
It is nonsuppurative condition, due to mumps.
Unilateral to start with, but in few days becomes bilateral, associated with constitutional disturbance.
Subacute & chronic parotitis:
It may be unilateral or bilateral.
Patient complains of recurrent swelling of parotid gland. Swelling particularly seen during meals.
The gland feels firmer, slightly tender & rubbery.
Diagnosis is confirmed if purulent saliva or watery saliva can be ejected from opening of the duct while gentle pressure is exerted over the gland.
Parotid tumors:
- Approximately 90% of neoplasms of salivary glands occurs in parotid glands, 10% in submandibular glands & very rarely in sublingual & ectopic salivary glands.
- Approximately 3/4th of epithelial lesions in the parotid are clearly benign, remaining 1/4th composed of definite carcinoma along with mucoepidermoid and acinic cell tumor which generally considered to be cancers of variable aggressiveness.
- In Submandibular gland majority of tumor are malignant.
- The most common cancers in salivary glands are in descending order of frequency-
- Muco-epidermoid tumors>adenoid cystic carcinoma>adenocarcinoma>epidermoid carcinoma>undifferentiated carcinoma>carcinoma arising in pleomorphic adenomas.




No comments:
Post a Comment